|
It has been six years since I last worked in the fields. I would migrate with my family from the Rio Valley Grande in Texas to various states across the Midwest to work in the onion and blueberry fields. One morning, while working at dawn in the onion field, I made a promise. I promised myself that I would finish college and make a difference in the lives of migrant agricultural workers that work the soil of this country and those who make it possible for Americans to have food on their table. I am proud to say that I am keeping true to my promise. I have been working at NCFH for over a year, developing health education tools that help agricultural workers better understand a health condition or how to get health care services. This October I was given the opportunity to attend, for the first time, the East Coast Migrant Stream Forum in Memphis, Tennessee. I was able to meet people who work in migrant health, from outreach workers to frontline staff working in a health center to CEO’s whose main goal is to improve the health and well-being of migratory and seasonal agricultural workers. During the three day conference, I participated in the exhibit letting everyone know about NCFH products and services. It was rewarding to see the appreciation that was given to the products and services that NCFH provides to health center staff. Furthermore, it was very rewarding to hear how these tools can really make a difference in the lives of agricultural workers. Throughout the Wall of Wonder (WOW) session, I along with almost 170 participants explored the issues of access to care for agricultural workers and strategies to increase access to care for them and their families. Participants were able to learn about the AG 2020 campaign , an effort to encourage health centers to take credit for all migratory and seasonal agricultural workers they serve, and how important this is in order to preserve the Migrant Health Program. Keynote speaker and U.S. Poet Laureate, Juan Felipe Herrera, reminded everyone that we all have a voice that is helping agricultural workers. He motivated us to continue doing the work that we do because it is much needed, but furthermore to keep our voice alive. He talked to us about his project La Casa de Colores, and expressed how this is a house for all voices and encouraged everyone to be part of it. I found this experience rewarding in many ways. It provided me with the opportunity to meet and learn from others that have been in the migrant health movement. It reminded me that the work that I do day to day is much appreciated and needed. This experience also reminded me about my promise and motivated me to continue helping our migrant agricultural workers. By: Joanna Arevalo 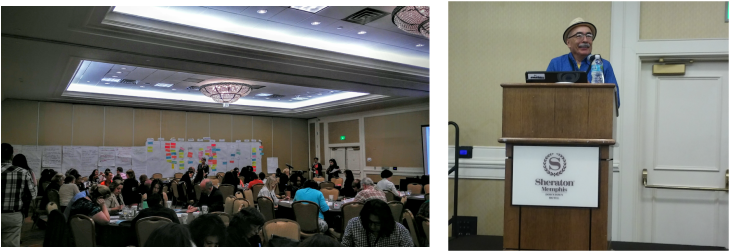 Photos:
Left -Wall of Wonder (W0W) Session at the East Coast Migrant Stream Forum 2015 Right- U.S. Poet Laureate, Juan Felipe Herrera, Keynote Speaker at East Coast Migrant Stream Forum 2015 Photo Credits: Joanna Arevalo  It is Health Literacy Month.
It’s alarming to think that only 12% of American adults are considered health literate, according to the National Assessment of Adult Illiteracy. In other words, nine out of ten Americans lack the basic knowledge to manage their health and prevent disease. This holds true for the vulnerable populations of our country, including migratory and seasonal agricultural workers. These populations face barriers to a basic understanding of their health and to receiving appropriate health education. Health Literacy – put simply – is one’s ability to understand and obtain health information. That is the simple definition. A much more complex definition resides in the specific factors and barriers contributing to a population’s lack of health literacy, which can correlate (not exclusively) to a person’s language, culture, location, and socioeconomic environment. Migratory and seasonal agricultural workers face unique obstacles to managing their own health care, including access to transportation to services, language barriers, and (in some cases) not being treated well due to undocumented status. When blockades exist to access to health, one’s access to health education will also be barricaded. Migrant and Community Health Centers strive for the elimination of health illiteracy among all their patients by providing preventive treatment and low literacy education materials for patients to learn more about a specific diagnosis or their risk factor(s). The patient is not solely responsible for his or her healthcare and health education. Health center staff are being trained to become culturally competent in their respective positions. Cultural competency – according to Health.gov – “is the ability of health organizations and practitioners to recognize the cultural beliefs, values, attitudes, traditions, language preferences, and health practices of diverse populations, and to apply that knowledge to produce a positive health outcome. Competency includes communicating in a manner that is linguistically and culturally appropriate.” NCFH prides itself on our ability to orient and train staff to implement cultural competency curriculums in the migrant and community health centers we serve. Participants of NCFH cultural competency courses learn to understand the meaning of diversity and its relationship and impact on communication and human relations. Along with that they increase awareness of their personal attitudes, beliefs and behaviors related to cultural diversity; and enhance skills for improved cross-cultural communication. NCFH also offers low literacy and English/Spanish translation services in order to continue improving a patient’s health literacy. Improving a health center staff’s cultural competence and patients' overall health literacy, allows for more involvement with, and awareness of, the diverse populations that health centers serve, and ultimately contributes toward eliminating one of the many barriers a patient faces related to health literacy. By: Mindy Morgan 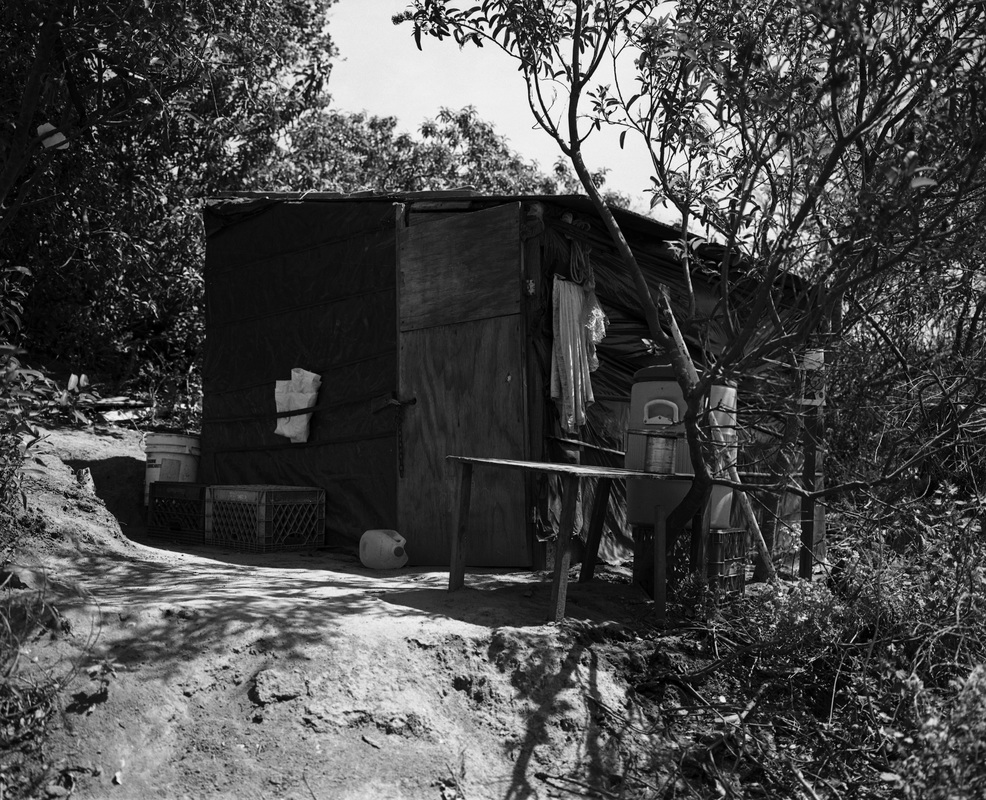 Behavioral and mental illness disorders remain part of a large conversation among the American public, and recent events make the need for depression and other mental health disorder screenings a must for health centers that serve the vulnerable communities in our country. Community Health Centers (CHCs) realize the very real concern of behavioral health issues among these populations. Nearly 70% of CHCs are screening for depression and other related mental health disorders around the nation, while 40% provide substance abuse counseling and treatment. According to the National Association of Community Health Centers (NACHC), “Persons living with mental illness have a higher mortality rate and often die prematurely due to preventable diseases such as: diabetes, cardiovascular disease, respiratory diseases, and infectious diseases.” The good news? There has been a dramatic growth in assessing the quality measures of behavioral health within the last decade. Although there is a growth in assessment, there is still work to be done. U.S. migrant and agricultural workers suffer with a higher susceptibility to the risks of behavioral health and its diagnosis. Migrant agricultural workers who are separated from their families may be more susceptible to mental health disorders, such as depression, alcoholism, and substance abuse. Nervios is a “culturally defined definition of stress.” A study conducted by National Agricultural Worker Survey (NAWS) reported that 20% of male agricultural workers experienced some form of Nervios and those who were separated from their families had reported a higher rate at 28%. When behavioral and mental health goes untreated, the results can be devastating on a personal and communal level. Many untreated disorders result in patient suicides, incarceration, homelessness and severe episodes of violence. To find a Community Health Center offering depression screening please visit: http://findahealthcenter.hrsa.gov/ By Mindy Morgan
Photo: Alan Pogue  Although there has been substantial progress in cancer treatment, screening, diagnosis, and prevention over the past several decades, addressing cancer health disparities—such as higher cancer death rates, less frequent use of proven screening tests, and higher rates of advanced cancer diagnoses—in certain populations is an area in which progress has not kept pace. These disparities are frequently seen in people from low-socioeconomic groups, certain racial/ethnic populations, and those who live in geographically isolated areas. – National Cancer Institute  The U.S. Latina population has lower-rates of breast cancer than non-Hispanic women. However, they have a 20% greater chance of dying than other women after receiving a positive diagnosis. Many attribute this discrepancy to the social determinants of health that influence patient survival – including a lack of access to quality education and healthcare, which is exacerbated by patients’ socioeconomic statuses. The unique seasonal and migratory lifestyles of female agricultural workers further compound and complicate these issues – as do the effects of existing misinformation regarding screenings and cultural beliefs amongst this population. The necessity of consistent appointments and follow-ups for effective care proves problematic for those on the move and those working under severe occupational time constraints. Women over the age of 50 are urged to get annual mammograms in addition to performing frequent self-examinations. However, a positive exam only constitutes an initial step in the breast cancer diagnosis process. Patients must return and provide a tissue sample before the disease is confirmed. Federally Qualified Health Centers (FQHCs) served more than 2 million women over the age of 50 and 440,000 women utilized services at Migrant Health Centers in 2014. FQHCs also performed more than 470,000 mammograms and found almost 110,000 breast abnormalities last year. The National Center for Farmworker Health recognizes the need for a special focus on breast cancer outreach to the U.S. female agricultural worker. Through its Cultivando la Salud program, NCFH offers health centers and other Hispanic-serving organizations the opportunity to receive train-the-trainer instruction intended to provide program planners with the knowledge, step-by-step process, and the tools to successfully plan and develop a comprehensive breast and cervical cancer education program for the agricultural population as well as other Hispanic communities. The training includes basic program planning information from designing the program goals and objectives to developing a budget to recruitment and training of lay health workers. The program also includes an evaluative component and specialized focus on the teaching tools lay health workers will be using in the community. At the end of the training, training participants will be provided with a complete training curriculum, a program manual to guide the implementation of the program, and the CLS teaching tools for lay health workers to use in the community. By Lindsey Bachman
Photo: Steve Debenport, iStock |
The National Center for Farmworker HealthImproving health care access for one of America's most vulnerable populations Archives
July 2024
Categories
All
|
 RSS Feed
RSS Feed